In development · for children who wet the bed
Measure bladder state, not wet fabric.
DryNight is a soft patch, worn low on the belly, being designed to sense bladder filling before wetness starts, cue your child privately, and bring you in only when it helps.
“My son wets the bed every night, the way I did as a boy. I am building what I wish we had.”
Stage
In development
Concept and feasibility planning. No finished device yet.
Who it is for
Children who wet the bed
Pediatric nocturnal enuresis first. No adult use until the pediatric work is done.
The hard problem
Overnight signal quality
Motion, posture, contact, power, comfort, false alerts, and useful lead time.
Next step
Feasibility testing
Test whether bladder filling can be estimated early enough to cue before voiding.
Concept-stage only. Not clinically validated, FDA-cleared, or available for diagnosis, treatment, or medical decision-making.

Photo: Obama Foundation ↗
The founder
I wet the bed until I was twelve.
I grew up in Cameroon. My grandparents tried everything: raw okra, anthills, every remedy the village knew. Nothing worked. I stopped going to boarding school so no one would find out. I became the cleanest, most driven student I could be, because I was convinced no one could ever know what I was hiding at night.
Now my nine-year-old son wets the bed every night. His is more severe than mine. I refuse to shame him the way I was shamed. But the best alarms on the market still have cords, still detect moisture after the fact, still fail him.
So I started building what I wish I had. DryNight begins with my son, but the standard is broader: a child should not have to be wet before the system understands that help is needed.
Ndansi Elvis Nukam
· Founder & CEO, DryNight01 · Problem
Most products react after the bed is already wet.
Moisture alarms can help some families, but they usually detect urine after it reaches clothing or bedding. DryNight starts from a different question: can a comfortable overnight patch estimate bladder filling early enough to cue before voiding?
-
Current alarms detect wetness
Moisture clips are useful for some families, but they begin after urine reaches clothing or bedding.
-
Clinical care still needs better home tools
Behavioral care, medication, and alarms all have roles. The missing product category is an earlier bladder-state signal that families can use at night.
-
Families need earlier information
The intended product is a quieter signal before the event, with caregiver escalation only when it helps.
Illustrative concept, not measured device output. The product question is whether that cue window can be detected reliably and comfortably overnight.
02 · Current solutions
Families already have options. None of them act before the bed is wet.
Bedwetting alarms, medication, behavioral programs, and existing bladder sensors each do real work. None of them gives a private cue at night, before voiding. That gap is the product DryNight is being built for.
| Approach | When it acts | What it asks of the family | The gap it leaves |
|---|---|---|---|
| Moisture alarms | After wetness reaches clothing or bedding | Weeks to months of consistent nightly use; tolerating a 2am alarm and laundry | Reacts to the event it is meant to prevent; many families stop before it works |
| Desmopressin | Reduces overnight urine production | A prescription, fluid limits, and management of relapse on stopping | Manages symptoms pharmacologically; relapse is common and it does not teach timing |
| Behavioral and urotherapy | Over weeks, through daytime habits and bladder training | Sustained effort from child and caregiver; clinic follow-up | Slow, effort-heavy, and not a nighttime signal |
| Daytime bladder sensors (SENS-U) | Notify when the bladder is near full, primarily for daytime urotherapy | Wearing and charging a lower-abdomen ultrasound sensor | Built around daytime full-bladder notification and urotherapy; the nocturnal pre-void cue remains unproven |
| DryNight (proposed) | During sleep, before voiding, at a chosen fill threshold | A comfortable patch and a private wrist cue; caregiver escalation only by plan | Unproven. This is the hypothesis DryNight has to earn through feasibility work. |
DryNight is concept-stage. The comparison describes intended product direction, not validated performance. The SENS-U row reflects a real commercial device; see the evidence room for citations.
03 · Night loop
You see the plan. Your child gets the first quiet cue.
The product is being designed around dignity first: the wearer, whether a child, an adult, or an older adult, gets a private signal before a caregiver is brought in.
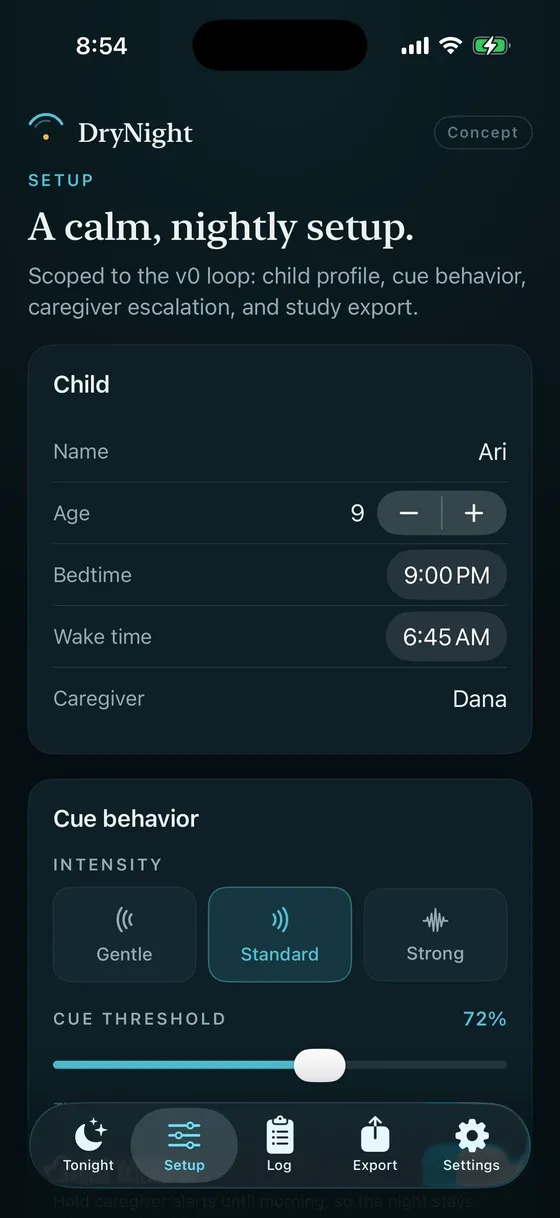
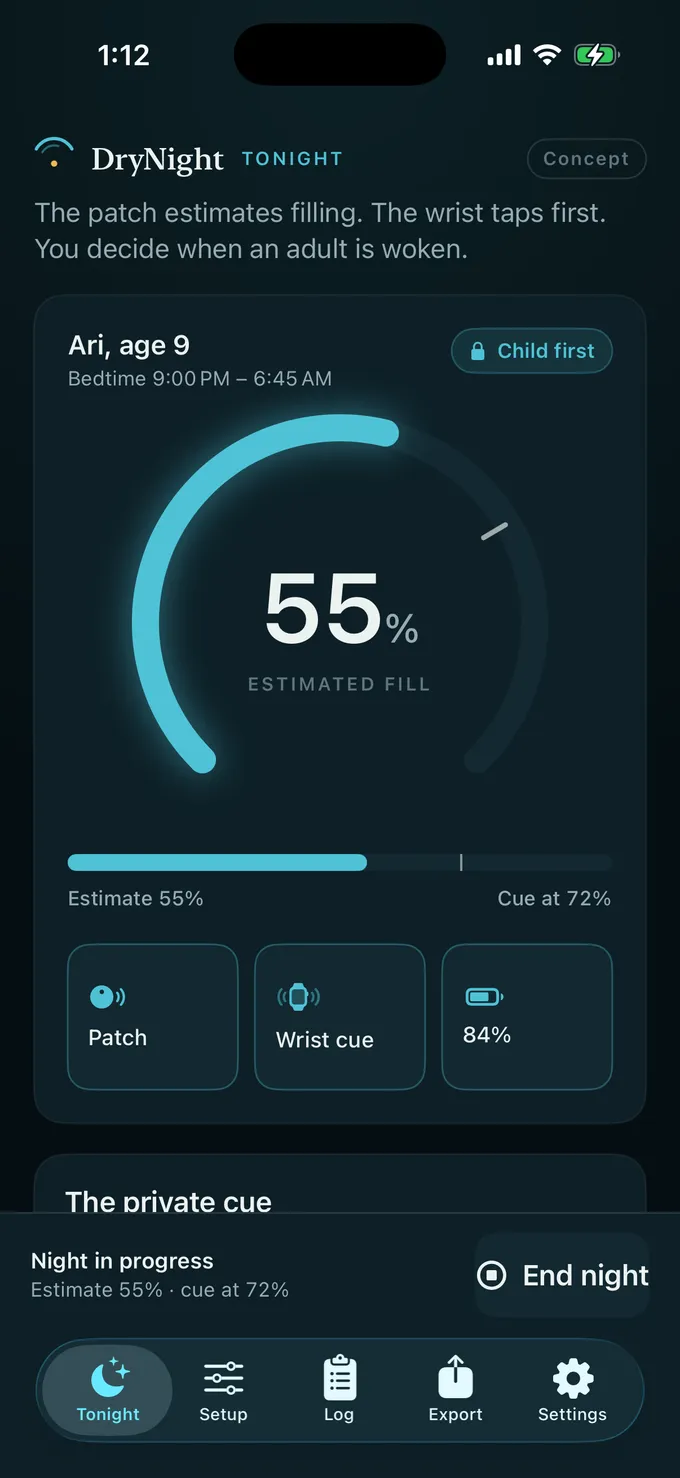
Profile, cue intensity, and escalation.

A live estimate of bladder filling on the sensing arc.
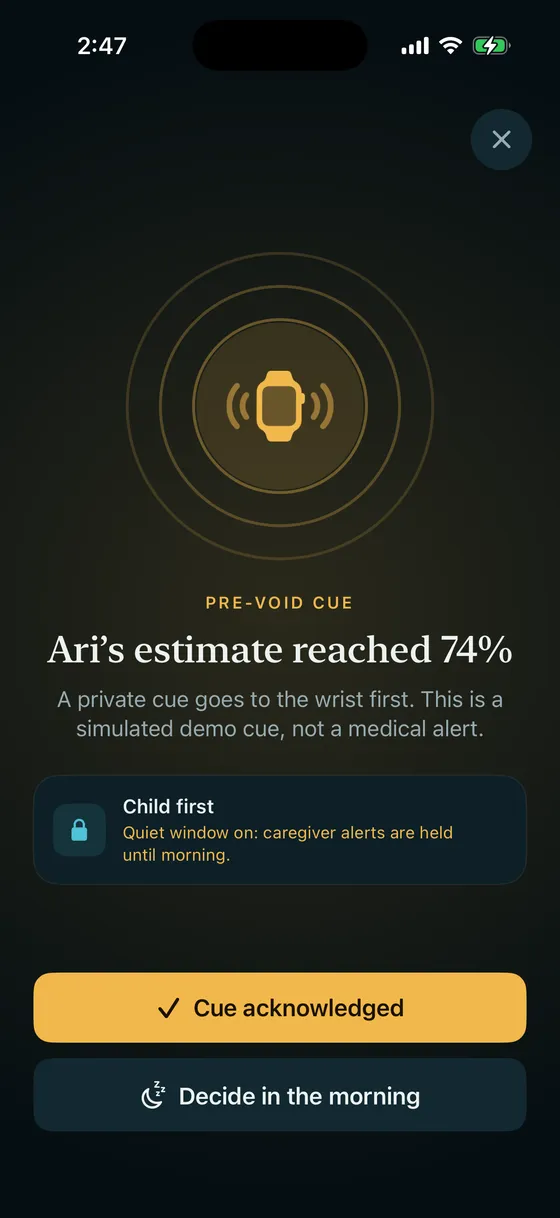
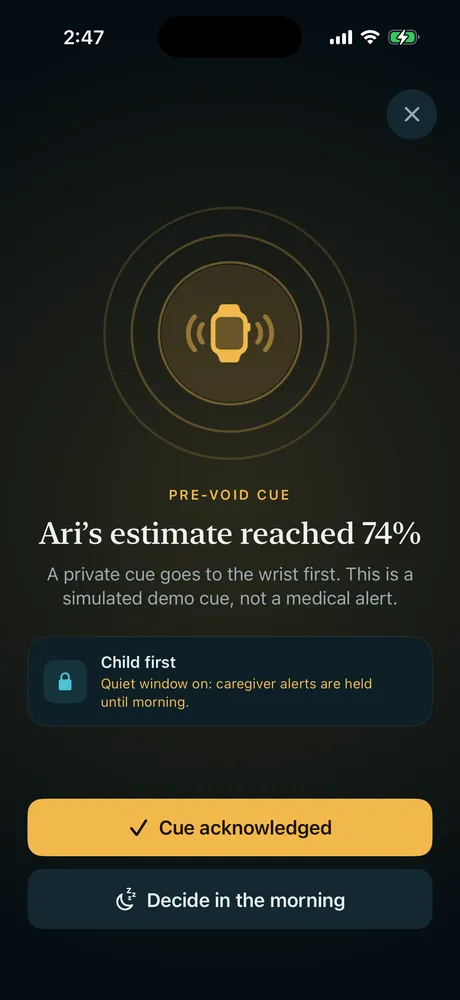
A private wrist cue first. Caregiver only if needed.
The loop, four moments.
-
01 Before bed
Place the patch once
The lower-abdomen patch has to be soft, cordless, and stable enough that setup does not become a nightly argument.
-
02 During sleep
Estimate bladder filling locally
Raw sensing should stay close to the device while the system looks for a conservative threshold, not a diagnostic conclusion.
-
03 First cue
Cue the wearer privately
The cue should be private and gentle before a public alarm or caregiver escalation is considered.
-
04 Escalation
Bring in help only when needed
Caregiver alerts should be configurable, minimal, and reserved for moments when the private cue alone is not enough.
The hardware path can change. These product standards should not.
-
Private by default
No loud bedroom alarm as the default interaction.
-
No claims before evidence
No performance numbers until a study supports them.
-
Comfort before dashboards
A family will not use a better signal if the device is hard to wear.
For families
The questions a parent actually asks.
Straight answers, including the ones that are still "we do not know yet."
Family list
Be the first to know when there is something to try.
One email. We write when there is real news, not before. No spam, no promises we cannot keep.
We will never share your address. This is not a medical service.
Is sensing my child’s belly every night safe? +
The lead approach is low-power ultrasound on the lower abdomen, related to sensors already used in children, but DryNight’s intended use is different: continuous, every-night, all-night sensing. That continuous use pattern is exactly what safety and human-factors work has to establish on its own; we do not assume it is safe because a daytime sensor exists. We will not ask a family to use it until that work is done and reviewed.
What would my child actually wear? +
The intended design is a soft patch on the lower abdomen and a wrist cue, not a cord clipped to pajamas. Comfort is treated as a primary product gate, because a better signal is useless if a child will not sleep in it.
Will it wake my child if they sleep through everything? +
Deep-sleep arousal is the hardest part of bedwetting and the reason many alarms fail. DryNight starts with a private, escalating wrist cue and lets caregivers decide when an adult is brought in. Whether the cue reliably rouses a child is one of the first things the feasibility studies have to answer.
When could we try it, and what might it cost? +
There is no product to buy yet and no date we would promise before the science supports it. The most useful thing right now is to leave your email so we can reach out when there is something real to try, and to tell us what the alarm years were actually like.
What can we do tonight, while you build? +
Talk to your pediatrician. Most childhood bedwetting resolves with time, and current options (alarms, desmopressin, and behavioral programs) help many families. DryNight is not a reason to delay care that could help your child now.
04 · Evidence room
Why we think this can work, and what still has to be proven.
Why the idea is plausible, where the first risk sits, and what has to be proven before any family is asked to trust it.
83%
of natural overnight bladder-filling cycles (15 of 18) were detected at home by the SENS-U in 14 children with enuresis, the setting closest to DryNight’s.
[1] Kwinten et al., 2020 ↗90%
of a controlled clinic urodynamic study (30 children, ages 6–12) had a full, catheter-filled bladder recognized before voiding by the SENS-U. A controlled-fill benchmark, not an overnight result.
[2] van Leuteren et al., 2018 ↗External findings, not DryNight performance data. They measure detection under different conditions, and in both studies the device only monitored: its alerts were switched off. Neither tested waking a child, so the hardest part of DryNight’s thesis (a cue that rouses a deep sleeper) has no precedent and must be earned.
Problem reality
Before any technical proof, the problem itself has to justify a better product: timing, dignity, and caregiver burden.
-
Bedwetting is common in school-age children and often resolves gradually rather than immediately. [3]
-
Most household alarms start only when wetting begins, long after the bladder first becomes actionable. [3][4]
-
Families need earlier information and less public interruption; a louder signal after wetness reaches clothing or bedding delivers neither. [4]
Technical precedent
Both studies below used a wearable ultrasound bladder sensor (the SENS-U), sold for daytime use in children. That a commercial device already estimates bladder state in this age group makes the sensing approach realistic. DryNight is building the overnight system that category has never attempted: the private cue, the escalation plan, and the home experience.
-
The SENS-U wearable ultrasound sensor detected full bladders before voiding in 90% of a 30-child urodynamic cohort aged 6 to 12. [2][6]
-
In a single-night home session, the SENS-U detected 83% of natural nocturnal bladder-filling cycles (15 of 18) in children with monosymptomatic nocturnal enuresis, without disturbing sleep. [1]
-
Noninvasive bladder monitoring is an active research area across ultrasound, bioimpedance, optical sensing, and flexible ultrasonic devices. [6][7]
Product thesis
The winning product here is a private timing system that fits the home. The sensor is only one part of it.
-
The first product is a soft lower-abdomen patch, a private wearer cue, and optional caregiver escalation.
-
The first milestone is timely pre-void cueing, before wetness starts.
-
The same timing problem can later support adult, older-adult, and caregiver workflows once the pediatric proof point is earned.
Validation milestones
This is the work between a strong idea and a product families can trust.
-
Select the sensing architecture that survives body-size variation, sleep position, motion, adhesion, and power constraints. [6][7]
-
Define an actionable threshold that balances missed cues, false cues, wearer comfort, and caregiver burden.
-
Run repeated-night usability and a clinician-reviewed pilot before expanding the market story. [3][4]
References
- [1] Continuous home monitoring of natural nocturnal bladder filling in children with nocturnal enuresis: a feasibility study · Kwinten et al., 2020 ↗
Single-night, at-home feasibility session in 14 children (of 15 enrolled) with monosymptomatic nocturnal enuresis. The SENS-U detected 83% of natural nocturnal bladder-filling cycles (15 of 18); the 3 missed cycles fell below the sensor’s volume detection limit. It did not disturb sleep.
- [2] Validation of a wearable ultrasonic bladder monitor in children during urodynamic studies · van Leuteren et al., 2018 ↗
Pediatric urodynamic-room study in 30 children aged 6 to 12. A wearable lower-abdomen ultrasound sensor detected the full bladder before voiding in 90% of patients (27 of 30). The device studied is the SENS-U (Novioscan).
- [3] Enuresis in Children: Common Questions and Answers · Lauters et al., 2022 ↗
Supports burden, spontaneous resolution, and the current standard of alarms plus desmopressin for many children.
- [4] Bedwetting in under 19s: initial treatment · NICE CG111, 2010 ↗
Clarifies that alarms detect when wetting starts, often require sustained family effort, and are not ideal for every household.
- [5] Management and treatment of nocturnal enuresis: an updated standardization document from the International Children's Continence Society · Nevéus et al., 2020 ↗
The ICCS standard separates enuresis into nocturnal polyuria (overnight output above 130% of expected bladder capacity, desmopressin-first), reduced nocturnal bladder capacity, and disordered arousal. It defines expected bladder capacity as (age + 1) x 30 mL and grounds why a pre-void cue fits some children, not all.
- [6] State of the Art of Non-Invasive Technologies for Bladder Monitoring: A Scoping Review · Hafid et al., 2023 ↗
Summarizes ultrasound, optical, and bioimpedance approaches for non-invasive bladder monitoring and highlights the field's current limits.
- [7] An integrated and flexible ultrasonic device for continuous bladder volume monitoring · Toymus et al., 2024 ↗
Shows that wearable ultrasound bladder sensing is technically plausible in research settings, while still distinct from a validated pediatric product.
- [8] Essity acquires smart ultrasound technology for incontinence care · Essity, April 2020 ↗
Hygiene company Essity acquired Novioscan, maker of the SENS-U pediatric bladder sensor, confirming the modality is a real commercial category, not only a research idea.
Deeper questions, including the investor FAQ and open advisory asks, live on the technology page.
05 · Market focus
Why pediatric bedwetting comes first.
DryNight starts with pediatric nocturnal enuresis because the pain is specific, recurring, and poorly served by existing consumer tools. Adult incontinence may follow, but the first proof has to be specific.
Pediatric nocturnal enuresis.
The first user is a child who can sleep through a full bladder and a parent trying to help without shame. The initial product experience should be private, comfortable, and small enough to test rigorously.
- Why here first
- Families already buy alarms, mattress protection, and repeated workarounds
- Validation path
- Bench testing, overnight usability, and pediatric continence input
Where this could help next
Long-term care and aging.
The same type of early bladder signal could eventually support older adults and caregivers. That market has different workflows, liability, staffing constraints, and reimbursement questions, so it belongs after pediatric feasibility.
- Why later
- Home care and long-term care once the signal is validated
- Validation path
- Workflow interviews before committing to a care-facility study
Public record
A record you can check.
Everything below is public and linkable: Elvis’s record in underserved care, global health leadership, and digital-health operations. It shows who is building this. It does not validate the device; that proof has to come from the studies.
- Origin
Healthcare access founder
Unite for Health describes Elvis building from frontline healthcare experience in Cameroon into the first Unite for Health micro-clinic. Columbia World Projects also lists him as Founder and President of Unite for Health Foundation, focused on access to basic healthcare in underserved communities.
- Selection
Obama Foundation Scholar
The Obama Foundation lists Ndansi Elvis Nukam in its 2018–2019 Columbia University Scholars cohort and identifies him as Founder and President of Unite for Health Foundation in Cameroon.
- Leadership
Mandela Washington Fellow
Wagner College profiled Elvis Ndansi Nukam during the Mandela Washington Fellowship and described his community-health work, nursing and public-health background, and plan to expand Unite for Health micro-clinics.
- Execution
Current digital-health operator
Carna Health publicly named Elvis Ndansi, MS, MPH, as Chief of Global Population Health in a 2024 leadership announcement for its kidney-care screening and monitoring platform.
- Continuity
Recent public healthcare profile
A later Obama Foundation alumni story lists Elvis as Chief of Global Population Health at Carna Health and Founder and President of Unite for Health Foundation, connecting the founder story to his current healthcare operating role.
Evidence boundary
- These sources establish founder operating context and a public track record in healthcare access.
- They do not validate DryNight’s sensor performance, clinical utility, or regulatory status.
- DryNight still has to earn product confidence through feasibility work, usability testing, clinical validation, and regulatory review.
Team
Right now, the team is one founder.
DryNight is Elvis's company, and the team is growing around the work, starting with the advisors the first study needs. Names will appear here when there is real permission and commitment behind them.
The seats to fill first
- 01 Pediatric urology or continence-study advisory leadership
- 02 Biomedical sensing and wearable engineering
- 03 Regulatory affairs (medical devices)
- 04 Quality, manufacturing, and supply-chain planning
Recognize yourself in one of these?
If you have run pediatric continence studies, shipped wearable sensors, or taken a device through the FDA, Elvis wants the conversation.
Talk to the founder →Contact
Help shape this while it is still early.
DryNight needs grounded input from families, clinicians, engineers, care operators, and investors while the concept becomes a device. Use this form for feedback, research conversations, partnership ideas, manufacturing leads, or funding conversations.
What happens next
Every note is read by Elvis. Follow-up happens when a real conversation would help, and your address never lands on a mailing list.
The fastest way to shape this product is to tell us where it would fail in your home, clinic, or facility.